What Is Overpronation
Overview
Overpronation is a term that gets thrown around a lot by psuedo-experts and there is so much written online about it, that it can get very confusing to determine what is legitimate and what is not. Pronation is a normal motion of the foot that occurs when the ankle rolls inwards and the arch collapses. This is normal. Its not something evil. Overpronation is assumed to be when there is too much of it. There certainly is debate as to just how much is too much, as some people have large amounts and have no problems, other have small amounts and do have problems. It all comes down to individual differences and how much force is needed to stop the foot moving. The greater the force, regardless of the amounts of pronation, the more likely it is to be a problem. Some still like to debate if it is a problem or not. Some studies have shown that its not a problem and other studies have shown it is. If the data from all these studies are pooled, then the conclusion was that, yes, overpronation is a problem that was statistically significant, but it was only a small risk factor for problems. An associated finding of overpronation during a gait analysis is an abductory twist.
Causes
There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis, achilles tendonopathy, hallus valgus and or bunions, patellofemoral pain syndrome, Iliotibial band pain syndrome, low back pain, shin splints, stress fractures in the foot or lower leg.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. This orthotics should be designed with appropriate arch support and medial rear foot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems. If the problem persists, consult your foot doctor.
Surgical Treatment
Hyperpronation can only be properly corrected by internally stabilizing the ankle bone on the hindfoot bones. Several options are available. Extra-Osseous TaloTarsal Stabilization (EOTTS) There are two types of EOTTS procedures. Both are minimally invasive with no cutting or screwing into bone, and therefore have relatively short recovery times. Both are fully reversible should complications arise, such as intolerance to the correction or prolonged pain. However, the risks/benefits and potential candidates vary. Subtalar Arthroereisis. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. HyProCure Implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%.
Overpronation is a term that gets thrown around a lot by psuedo-experts and there is so much written online about it, that it can get very confusing to determine what is legitimate and what is not. Pronation is a normal motion of the foot that occurs when the ankle rolls inwards and the arch collapses. This is normal. Its not something evil. Overpronation is assumed to be when there is too much of it. There certainly is debate as to just how much is too much, as some people have large amounts and have no problems, other have small amounts and do have problems. It all comes down to individual differences and how much force is needed to stop the foot moving. The greater the force, regardless of the amounts of pronation, the more likely it is to be a problem. Some still like to debate if it is a problem or not. Some studies have shown that its not a problem and other studies have shown it is. If the data from all these studies are pooled, then the conclusion was that, yes, overpronation is a problem that was statistically significant, but it was only a small risk factor for problems. An associated finding of overpronation during a gait analysis is an abductory twist.
Causes
There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis, achilles tendonopathy, hallus valgus and or bunions, patellofemoral pain syndrome, Iliotibial band pain syndrome, low back pain, shin splints, stress fractures in the foot or lower leg.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. This orthotics should be designed with appropriate arch support and medial rear foot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems. If the problem persists, consult your foot doctor.
Surgical Treatment
Hyperpronation can only be properly corrected by internally stabilizing the ankle bone on the hindfoot bones. Several options are available. Extra-Osseous TaloTarsal Stabilization (EOTTS) There are two types of EOTTS procedures. Both are minimally invasive with no cutting or screwing into bone, and therefore have relatively short recovery times. Both are fully reversible should complications arise, such as intolerance to the correction or prolonged pain. However, the risks/benefits and potential candidates vary. Subtalar Arthroereisis. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. HyProCure Implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%.
How You Can Diagnose Calcaneal Apophysitis?
Overview
Sever?s disease or Sever?s lesion refers to an injury to the bone growth plate at the back of the heel bone (calcaneous) in young people, particularly those who are physically active. It usually develops in puberty and is slightly more common in boys than girls.
Causes
Physically active children run the risk of developing Sever?s disease because they put the most strain on their growing bones. Sever?s usually occurs during the adolescent growth spurt, when young people grow most rapidly. (This growth spurt can begin any time between the ages of 8 and 13 for girls and 10 and 15 for boys.) By age 15 the back of the heel usually finished growing. As teens grow, the growth plates harden and the growing bones fuse together into mature bone. Young people engaged in physical activities and sports that involve jumping and running on hard surfaces-such as track, basketball, soccer, and gymnastics-are ata higher risk for developing Sever?s disease. Poor-fitting shoes can contribute by not providing enough support or padding for the feet or by rubbing against the back of the heel.
Symptoms
Symptoms of calcaneal apophysitis may include Pain in the back or bottom of the heel, Limping, Walking on toes, Difficulty running, jumping, or participating in usual activities or sports, Pain when the sides of the heel are squeezed.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
Depending on the diagnosis and the severity of the pain, there a number of treatment options available. Rest, reduce activity, your child should reduce or stop any activity that causes pain, such as sports and running. This can be a difficult option, as children are normally quite willful in pursuit of their favorite pastimes. Over the counter anti-inflammatory drugs, such as ibuprofen (found in Nurofen), to help reduce pain and inflammation. Make certain your child does stretching exercises before play. This will often help reduce the stress on the fascia and relieve heel pain in your child. Orthotic insoles. Orthotics made for children will help support the foot properly, and help prevent over-pronation or improper gait by supporting your child?s foot into a proper biomechanical position. Do not hesitate to schedule an appointment with a podiatrist, should your child?s heel and foot pain persist.
Sever?s disease or Sever?s lesion refers to an injury to the bone growth plate at the back of the heel bone (calcaneous) in young people, particularly those who are physically active. It usually develops in puberty and is slightly more common in boys than girls.
Causes
Physically active children run the risk of developing Sever?s disease because they put the most strain on their growing bones. Sever?s usually occurs during the adolescent growth spurt, when young people grow most rapidly. (This growth spurt can begin any time between the ages of 8 and 13 for girls and 10 and 15 for boys.) By age 15 the back of the heel usually finished growing. As teens grow, the growth plates harden and the growing bones fuse together into mature bone. Young people engaged in physical activities and sports that involve jumping and running on hard surfaces-such as track, basketball, soccer, and gymnastics-are ata higher risk for developing Sever?s disease. Poor-fitting shoes can contribute by not providing enough support or padding for the feet or by rubbing against the back of the heel.
Symptoms
Symptoms of calcaneal apophysitis may include Pain in the back or bottom of the heel, Limping, Walking on toes, Difficulty running, jumping, or participating in usual activities or sports, Pain when the sides of the heel are squeezed.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
Depending on the diagnosis and the severity of the pain, there a number of treatment options available. Rest, reduce activity, your child should reduce or stop any activity that causes pain, such as sports and running. This can be a difficult option, as children are normally quite willful in pursuit of their favorite pastimes. Over the counter anti-inflammatory drugs, such as ibuprofen (found in Nurofen), to help reduce pain and inflammation. Make certain your child does stretching exercises before play. This will often help reduce the stress on the fascia and relieve heel pain in your child. Orthotic insoles. Orthotics made for children will help support the foot properly, and help prevent over-pronation or improper gait by supporting your child?s foot into a proper biomechanical position. Do not hesitate to schedule an appointment with a podiatrist, should your child?s heel and foot pain persist.
Treatment And Cause
Overview
One in four adults in the U.S. has adult acquired flatfoot deformity, which may begin during childhood or be acquired with age. The foot may be flat all the time or may lose its arch when the person stands. The most common and serious cause of flat foot is Posterior Tibial Tendon Dysfunction, in which the main tendon that supports the arch gradually weakens. 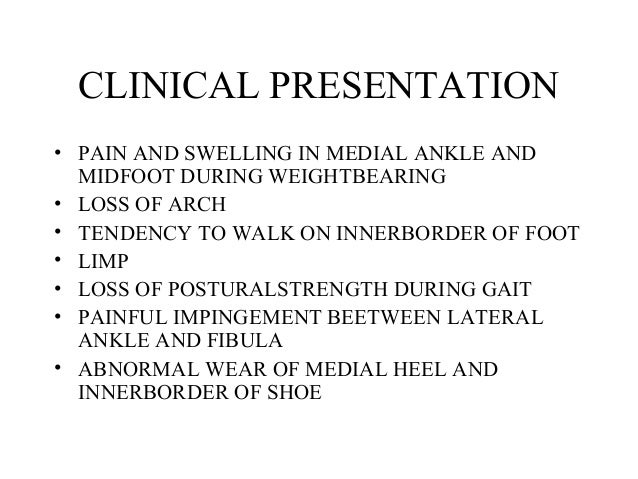
Causes
There are numerous causes of acquired Adult Flatfoot, including, trauma, fracture, dislocation, tendon rupture/partial rupture or inflammation of the tendons, tarsal coalition, arthritis, neuroarthropathy and neurologic weakness. The most common cause of acquired Adult Flatfoot is due to overuse of a tendon on the inside of the ankle called the posterior tibial tendon. This is classed as - posterior tibial tendon dysfunction. What are the causes of Adult Acquired flat foot? Trauma, Fracture or dislocation. Tendon rupture, partial tear or inflammation. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain.
Diagnosis
Although you can do the "wet test" at home, a thorough examination by a doctor will be needed to identify why the flatfoot developed. Possible causes include a congenital abnormality, a bone fracture or dislocation, a torn or stretched tendon, arthritis or neurologic weakness. For example, an inability to rise up on your toes while standing on the affected foot may indicate damage to the posterior tibial tendon (PTT), which supports the heel and forms the arch. If "too many toes" show on the outside of your foot when the doctor views you from the rear, your shinbone (tibia) may be sliding off the anklebone (talus), another indicator of damage to the PTT. Be sure to wear your regular shoes to the examination. An irregular wear pattern on the bottom of the shoe is another indicator of acquired adult flatfoot. Your physician may request X-rays to see how the bones of your feet are aligned. Muscle and tendon strength are tested by asking you to move the foot while the doctor holds it.
Non surgical Treatment
A painless flatfoot that does not hinder your ability to walk or wear shoes requires no special treatment or orthotic device. Other treatment options depend on the cause and progression of the flatfoot. Conservative treatment options include making shoe modifications. Using orthotic devices such as arch supports and custom-made orthoses. Taking nonsteroidal anti-inflammatory drugs such as ibuprofen to relieve pain. Using a short-leg walking cast or wearing a brace. Injecting a corticosteroid into the joint to relieve pain. Rest and ice. Physical therapy. In some cases, surgery may be needed to correct the problem. Surgical procedures can help reduce pain and improve bone alignment. 
Surgical Treatment
Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss.
Pain In The Arches All You Need To Know
Overview
Flexible flatfeet are considered normal in young children because babies are not born with a normal arch. The arch may not form fully until sometime between ages 7 and 10. Even in adulthood, 15% to 25% of people have flexible flatfeet. Most of these people never develop symptoms. In many adults who have had flexible flatfeet since childhood, the missing arch is an inherited condition related to a general looseness of ligaments. These people usually have extremely flexible, very mobile joints throughout the body, not only in the feet. Flatfeet also can develop during adulthood. Causes include joint disease, such as rheumatoid arthritis, and disorders of nerve function (neuropathy).

Causes
A common cause of foot arch pain is a stress fracture. They tend to occur from repeated overloading of one of the foot bones from activities such as jumping and running especially if you have suddenly increased your activity level. The breaks in the bone may be small but they can be extremely painful. Stress fractures of the metatarsal bones or the navicular can cause anything from mild to severe foot arch pain. The Tibialis Posterior muscle plays a very important role in supporting the medial arch of the foot. Posterior Tibial Tendonitis can occur either through repetitive use e.g. high impact sports such as soccer or tennis, or from an injury e.g. a fall. This causes the tendon to become inflamed or even torn, resulting in pain on bottom of foot. This pain usually gets worse with activity or when standing for long periods. If the problem persists, the inner side of the foot (known as the medial longitudinal arch of the foot) gradually collapses down, causing flat feet. A simple test for this condition is to stand on one leg and rise up onto your tiptoes. If you cannot, it indicates a problem with the Posterior Tibial tendon. Treatment usually consists of rest, ice, exercises, orthotics and physical therapy.
Symptoms
Repetitive exertive activity arch pain is usually sharp, and localized to a specific area, rather than the entire arch. Usually the pain occurs in the area just in front of the heel. It is present when first standing on the foot in the morning, but may decrease once you start walking around, but will, gradually becomes worse with continued walking or running. Swelling may be present. The pain subsides with rest, but stretching the arch while resting may cause the pain to return. Injury pain is constantly present, but worse when standing on the foot. This pain is localized to a specific area, but may radiate out from this area to the entire foot. The pain is sharp, and usually accompanied by swelling and occasionally "black and blue" discolorations. The pain due to the natural aging process is usually dull and aching, or stiff, and can be felt throughout the entire arch area, rather then in just one spot. This pain is present whenever weight bearing, and usually becomes worse with continued walking. The pain gradually subsides when resting, and usually does not return with stretching. Biomechanical defect pain is usually localized to a section of the arch, such as the inner, middle, outer, front, or back of the arch. This pain may be sharp or dull, but is always worse with continued walking.
Diagnosis
To come to a correct diagnosis, your podiatrist will examine your foot by using his or her fingers to look for a lump or stone bruise in the ball of your foot. He or she will examine your foot to look for deformities such as high or low arches, or to see if you have hammertoes. He or she may use x-rays, MRIs (magnetic resource imaging), and CT scans to rule out fractures and damage to ligaments, tendons, and other surrounding tissues. Your doctor will also inquire about your daily activities, symptoms, medical history, and family history. If you spend a lot of time running or jumping, you may be at a higher risk for pain in the bottom of your foot. These diagnostic tests will help your doctor come to a proper diagnosis and create an appropriate treatment plan.
Non Surgical Treatment
Stretch the fascia. Prop your toes up against a wall, keeping your arch and heel flat so the toes stretch. Hold for a count of 10. Repeat 10 times three or four times per day. Roll a frozen water bottle under the arch. Stretch first then roll out the arch for 10 minutes; you don?t want to stretch the tendon when it?s ice cold. Freeze a golf ball and massage the fascia. Roll the frozen golf ball under the foot, starting from the front and working your way back. Put good pressure on each spot-the medial, center and lateral positions-for 15 seconds before moving to the next area. Then, roll the ball back and forth over the entire foot. Foam roll all muscles on the body above the plantar. Even tight shoulders can cause the condition, as your arm swing can throw off proper hip alignment and footstrike. Bump your arch. Get a commercial insole with an arch bump to push on the plantar and keep it from flexing-it doesn?t matter if you?re an under or overpronator; the plantar needs to be supported and strengthened, Wear the support in all shoes, if possible.

Surgical Treatment
The main goal of surgery is to reduce pain and improve function. It may also reduce other injuries such as repeated ankle sprains and broken bones. Surgery may be considered if there is no relief with physical therapy, changes in shoewear and/or changes in activity. Some patients will also have tendon problems, ankle weakness and foot fractures. These patients may require other procedures to address related problems. If you have medical problems that make surgery unsafe, any infections or blood vessel disease, cavus foot surgery may not be appropriate. The surgical procedures involved with the correction of the cavus foot are varied. Theses may include correction of the bony deformity, ankle looseness and the muscle imbalances that cause the deformity. The goal is to provide a foot that evenly distributes weight along both inside and outside edges. A variety of incisions may be needed to perform the procedures related to the correction of the cavus foot.
Prevention
Stretch and strengthen important muscles in your feet, ankles and legs in order to guard against future strain. Make sure to acquire suitable arch supports and inserts if necessary, and that your shoes are shock absorbent and in good condition. Wearing tattered shoes provides no protection, and runners should replace their footwear before exceeding 500 miles of usage. Athletes new to arch supports should gradually build their training routine, allowing their feet to become accustomed to a new stance.
Flexible flatfeet are considered normal in young children because babies are not born with a normal arch. The arch may not form fully until sometime between ages 7 and 10. Even in adulthood, 15% to 25% of people have flexible flatfeet. Most of these people never develop symptoms. In many adults who have had flexible flatfeet since childhood, the missing arch is an inherited condition related to a general looseness of ligaments. These people usually have extremely flexible, very mobile joints throughout the body, not only in the feet. Flatfeet also can develop during adulthood. Causes include joint disease, such as rheumatoid arthritis, and disorders of nerve function (neuropathy).
Causes
A common cause of foot arch pain is a stress fracture. They tend to occur from repeated overloading of one of the foot bones from activities such as jumping and running especially if you have suddenly increased your activity level. The breaks in the bone may be small but they can be extremely painful. Stress fractures of the metatarsal bones or the navicular can cause anything from mild to severe foot arch pain. The Tibialis Posterior muscle plays a very important role in supporting the medial arch of the foot. Posterior Tibial Tendonitis can occur either through repetitive use e.g. high impact sports such as soccer or tennis, or from an injury e.g. a fall. This causes the tendon to become inflamed or even torn, resulting in pain on bottom of foot. This pain usually gets worse with activity or when standing for long periods. If the problem persists, the inner side of the foot (known as the medial longitudinal arch of the foot) gradually collapses down, causing flat feet. A simple test for this condition is to stand on one leg and rise up onto your tiptoes. If you cannot, it indicates a problem with the Posterior Tibial tendon. Treatment usually consists of rest, ice, exercises, orthotics and physical therapy.
Symptoms
Repetitive exertive activity arch pain is usually sharp, and localized to a specific area, rather than the entire arch. Usually the pain occurs in the area just in front of the heel. It is present when first standing on the foot in the morning, but may decrease once you start walking around, but will, gradually becomes worse with continued walking or running. Swelling may be present. The pain subsides with rest, but stretching the arch while resting may cause the pain to return. Injury pain is constantly present, but worse when standing on the foot. This pain is localized to a specific area, but may radiate out from this area to the entire foot. The pain is sharp, and usually accompanied by swelling and occasionally "black and blue" discolorations. The pain due to the natural aging process is usually dull and aching, or stiff, and can be felt throughout the entire arch area, rather then in just one spot. This pain is present whenever weight bearing, and usually becomes worse with continued walking. The pain gradually subsides when resting, and usually does not return with stretching. Biomechanical defect pain is usually localized to a section of the arch, such as the inner, middle, outer, front, or back of the arch. This pain may be sharp or dull, but is always worse with continued walking.
Diagnosis
To come to a correct diagnosis, your podiatrist will examine your foot by using his or her fingers to look for a lump or stone bruise in the ball of your foot. He or she will examine your foot to look for deformities such as high or low arches, or to see if you have hammertoes. He or she may use x-rays, MRIs (magnetic resource imaging), and CT scans to rule out fractures and damage to ligaments, tendons, and other surrounding tissues. Your doctor will also inquire about your daily activities, symptoms, medical history, and family history. If you spend a lot of time running or jumping, you may be at a higher risk for pain in the bottom of your foot. These diagnostic tests will help your doctor come to a proper diagnosis and create an appropriate treatment plan.
Non Surgical Treatment
Stretch the fascia. Prop your toes up against a wall, keeping your arch and heel flat so the toes stretch. Hold for a count of 10. Repeat 10 times three or four times per day. Roll a frozen water bottle under the arch. Stretch first then roll out the arch for 10 minutes; you don?t want to stretch the tendon when it?s ice cold. Freeze a golf ball and massage the fascia. Roll the frozen golf ball under the foot, starting from the front and working your way back. Put good pressure on each spot-the medial, center and lateral positions-for 15 seconds before moving to the next area. Then, roll the ball back and forth over the entire foot. Foam roll all muscles on the body above the plantar. Even tight shoulders can cause the condition, as your arm swing can throw off proper hip alignment and footstrike. Bump your arch. Get a commercial insole with an arch bump to push on the plantar and keep it from flexing-it doesn?t matter if you?re an under or overpronator; the plantar needs to be supported and strengthened, Wear the support in all shoes, if possible.
Surgical Treatment
The main goal of surgery is to reduce pain and improve function. It may also reduce other injuries such as repeated ankle sprains and broken bones. Surgery may be considered if there is no relief with physical therapy, changes in shoewear and/or changes in activity. Some patients will also have tendon problems, ankle weakness and foot fractures. These patients may require other procedures to address related problems. If you have medical problems that make surgery unsafe, any infections or blood vessel disease, cavus foot surgery may not be appropriate. The surgical procedures involved with the correction of the cavus foot are varied. Theses may include correction of the bony deformity, ankle looseness and the muscle imbalances that cause the deformity. The goal is to provide a foot that evenly distributes weight along both inside and outside edges. A variety of incisions may be needed to perform the procedures related to the correction of the cavus foot.
Prevention
Stretch and strengthen important muscles in your feet, ankles and legs in order to guard against future strain. Make sure to acquire suitable arch supports and inserts if necessary, and that your shoes are shock absorbent and in good condition. Wearing tattered shoes provides no protection, and runners should replace their footwear before exceeding 500 miles of usage. Athletes new to arch supports should gradually build their training routine, allowing their feet to become accustomed to a new stance.
Posterior Tibial Tendon Dysfunction (PTTD)
Overview
Posterior tibial tendon dysfunction (PTTD) is an inflammation and / or overstretching of the posterior tibial tendon in the foot. An important function of the posterior tibial tendon is to help support the arch. But in PTTD, the tendon?s ability to perform that job is impaired, often resulting in a flattening of the foot. PTTD is often called ?adult-acquired flatfoot? because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. PTTD is usually progressive, which means it will keep getting worse-especially if it isn?t treated early. This differs from flexible flatfoot because flexible flatfoot typically begins in childhood or adolescence and continues into adulthood. It usually occurs in both feet and generally progresses in severity throughout the adult years. As the deformity worsens, the soft tissues (tendons and ligaments) of the arch may stretch or tear and become inflamed. The term ?flexible? means that while the foot is flat when standing (weight bearing), the arch returns when not standing. In the early stages of flexible flatfoot arthritis is not restricting motion of the arch and foot, but in the later stages arthritis may develop to such a point that the arch and foot become stiff. 
Causes
The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction. What causes adult acquired flat foot? Fracture or dislocation. Tendon laceration. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
In many cases, adult flatfoot causes no pain or problems. In others, pain may be severe. Many people experience aching pain in the heel and arch and swelling along the inner side of the foot.
Diagnosis
Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot.
Non surgical Treatment
Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities. In many cases of PTTD, treatment can begin with non-surgical approaches that may include orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support.
Surgical Treatment
If conservative treatment fails to provide relief of pain and disability then surgery is considered. Numerous factors determine whether a patient is a surgical candidate. They include age, obesity, diabetes, vascular status, and the ability to be compliant with post-operative care. Surgery usually requires a prolonged period of nonweightbearing immobilization. Total recovery ranges from 3 months to one year. Clinical, x-ray, and MRI examination are all used to select the appropriate surgical procedure.
Treating Flat Feet In Adults
Overview
Most flat feet are not painful, particularly those flat feet seen in children. In the adult acquired flatfoot, pain occurs because soft tissues (tendons and ligaments) have been torn. The deformity progresses or worsens because once the vital ligaments and posterior tibial tendon are lost, nothing can take their place to hold up the arch of the foot. The painful, progressive adult acquired flatfoot affects women four times as frequently as men. It occurs in middle to older age people with a mean age of 60 years. Most people who develop the condition already have flat feet. A change occurs in one foot where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Why this event occurs in some people (female more than male) and only in one foot remains poorly understood. Contributing factors increasing the risk of adult acquired flatfoot are diabetes, hypertension, and obesity. 
Causes
There are numerous causes of acquired Adult Flatfoot, including, trauma, fracture, dislocation, tendon rupture/partial rupture or inflammation of the tendons, tarsal coalition, arthritis, neuroarthropathy and neurologic weakness. The most common cause of acquired Adult Flatfoot is due to overuse of a tendon on the inside of the ankle called the posterior tibial tendon. This is classed as - posterior tibial tendon dysfunction. What are the causes of Adult Acquired flat foot? Trauma, Fracture or dislocation. Tendon rupture, partial tear or inflammation. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
The first stage represents inflammation and symptoms originating from an irritated posterior tibial tendon, which is still functional. Stage two is characterized by a change in the alignment of the foot noted on observation while standing (see above photos). The deformity is supple meaning the foot is freely movable and a ?normal? position can be restored by the examiner. Stage two is also associated with the inability to perform a single-leg heel rise. The third stage is dysfunction of the posterior tibial tendon is a flatfoot deformity that becomes stiff because of arthritis. Prolonged deformity causes irritation to the involved joints resulting in arthritis. The fourth phase is a flatfoot deformity either supple (stage two) or stiff (stage 3) with involvement of the ankle joint. This occurs when the deltoid ligament, the major supporting structure on the inside of the ankle, fails to provide support. The ankle becomes unstable and will demonstrate a tilted appearance on X-ray. Failure of the deltoid ligament results from an inward displacement of the weight bearing forces. When prolonged, this change can lead to ankle arthritis. The vast majority of patients with acquired adult flatfoot deformity are stage 2 by the time they seek treatment from a physician.
Diagnosis
Perform a structural assessment of the foot and ankle. Check the ankle for alignment and position. When it comes to patients with severe PTTD, the deltoid has failed, causing an instability of the ankle and possible valgus of the ankle. This is a rare and difficult problem to address. However, if one misses it, it can lead to dire consequences and potential surgical failure. Check the heel alignment and position of the heel both loaded and during varus/valgus stress. Compare range of motion of the heel to the normal contralateral limb. Check alignment of the midtarsal joint for collapse and lateral deviation. Noting the level of lateral deviation in comparison to the contralateral limb is critical for surgical planning. Check midfoot alignment of the naviculocuneiform joints and metatarsocuneiform joints both for sag and hypermobility.
Non surgical Treatment
Get treated early. There is no recommended home treatment. While in stage one of the deformity, rest, a cast, and anti-inflammatory therapy can help you find relief. This treatment is followed by creating custom-molded foot orthoses and orthopedic footwear. These customized items are critical in maintaining the stability of the foot and ankle. Once the tendon has stretched and deformity is visible, the chances of success for non-surgical treatment are significantly lower. In a small percentage of patients, total immobilization may arrest the progression of the deformity. A long-term brace known as an ankle foot orthosis is required to keep the deformity from progressing. The Richie Brace, a type of ankle foot orthosis, shows significant success as a treatment for stage two posterior tibial dysfunction. It is a sport-style brace connected to a custom corrected foot orthodic that fits into most lace-up footwear (including athletic shoes). It is also light weight and more cosmetically appealing than traditionally prescribed ankle foot orthosis. The Arizona Brace, California Brace or Gauntlet Brace may also be recommended depending on your needs. 
Surgical Treatment
Surgery should only be done if the pain does not get better after a few months of conservative treatment. The type of surgery depends on the stage of the PTTD disease. It it also dictated by where tendonitis is located and how much the tendon is damaged. Surgical reconstruction can be extremely complex. Some of the common surgeries include. Tenosynovectomy, removing the inflamed tendon sheath around the PTT. Tendon Transfer, to augment the function of the diseased posterior tibial tendon with a neighbouring tendon. Calcaneo-osteotomy, sometimes the heel bone needs to be corrected to get a better heel bone alignment. Fusion of the Joints, if osteoarthritis of the foot has set in, fusion of the joints may be necessary.
Insertional Achilles Tendonitis Massage
Overview
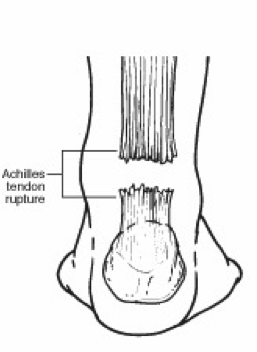 Achilles tendinitis is an irritation/inflammation in the achilles tendon, which attaches to the back of the heel. It is often a result of overuse and occurs frequently in runners who have altered their training suddenly, either with regard to duration or intensity. This injury is also prevalent in middle-aged people who are active.
Achilles tendinitis is an irritation/inflammation in the achilles tendon, which attaches to the back of the heel. It is often a result of overuse and occurs frequently in runners who have altered their training suddenly, either with regard to duration or intensity. This injury is also prevalent in middle-aged people who are active.
Causes
There are a number of ways a person can develop Achilles tendinitis. Some causes are easier to avoid than others, but being aware of them can aid earlier diagnosis and help prevent serious injury. Causes of Achilles tendinitis include, using incorrect or worn out shoes when running or exercising. Not warming up properly before exercise. Increasing intensity of exercise too quickly (e.g. running speed or distance covered). Prematurely introducing hill running or stair climbing to exercise routine. Running on hard or uneven surfaces. Calf muscle is injured or has little flexibility (this puts a lot of strain on the Achilles tendon). Sudden intense physical activity such as sprinting for the finish line. Achilles tendinitis can also be caused by differences in foot, leg or ankle anatomy. For example, some people can have flatness in their foot where there would normally be an arch; this puts more strain on the tendon. The FDA has asked that a boxed warning be added to the prescribing information for fluoroquinolone antibiotics. Patients taking these drugs may experience an increased risk of tendinitis and tendon rupture. Fluoroquinolones include Cipro (ciprofloxacin), Factive (gemifloxacin), Levaquin (levofloxacin), Avelox (moxifloxacin), Noroxin (norfloxacin), Floxin (ofloxacin) and Proquin (ciprofloxacin hydrochloride). It is important to remember that the risk for injury is not necessarily gone when the drug is stopped. Cases have been reported in which tendon problems occurred up to several months after the drug was discontinued.
Symptoms
Symptoms of Achilles tendinitis and tendinosis include recurring localized heel pain, sometimes severe, along the achilles tendon during or after exercise. Pain often begins after exercise and gradually worsens. Morning tenderness or stiffness about an inch and a half above the point where the Achilles tendon is attached to the heel bone. Sluggishness in your leg. Mild to severe swelling. Stiffness that generally diminishes as the tendon warms up with use.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
Most of the time, treatment for achilles tendinitis beginning with nonsurgical options. Your CFO physician may recommend rest, ice, ibuprofen, and physical therapy. If after 6 months, the pain does not improve, surgical treatment may be necessary. The type of surgery would depend on the exact location of the tendinitis and extent of damage.

Surgical Treatment
Surgery for an Achilles tendon rupture can be done with a single large incision, which is called open surgery. Or it can be done with several small incisions. This is called percutaneous surgery. The differences in age and activity levels of people who get surgery can make it hard to know if Achilles tendon surgery is effective. The success of your surgery can depend on, your surgeon's experience. The type of surgery you have. How damaged the tendon is. How soon after rupture the surgery is done. How soon you start your rehab program after surgery. How well you follow your rehab program. Talk to your surgeon about his or her surgical experience. Ask about his or her success rate with the technique that would best treat your condition.
Prevention
Achilles tendinitis cannot always be prevented but the following tips will help you reduce your risk. If you are new to a sport, gradually ramp up your activity level to your desired intensity and duration. If you experience pain while exercising, stop. Avoid strenuous activity that puts excessive stress on your Achilles tendon. If you have a demanding workout planned, warm up slowly and thoroughly. Always exercise in shoes that are in good condition and appropriate for your activity or sport. Be sure to stretch your calf muscles and Achilles tendon before and after working out. If you suffer from Achilles tendinitis make sure you treat it properly and promptly. If self-care techniques don?t work, don?t delay. Book a consultation with a foot care expert or you may find yourself sidelined from your favourite sports and activities.
Achilles tendinitis is an irritation/inflammation in the achilles tendon, which attaches to the back of the heel. It is often a result of overuse and occurs frequently in runners who have altered their training suddenly, either with regard to duration or intensity. This injury is also prevalent in middle-aged people who are active.
Causes
There are a number of ways a person can develop Achilles tendinitis. Some causes are easier to avoid than others, but being aware of them can aid earlier diagnosis and help prevent serious injury. Causes of Achilles tendinitis include, using incorrect or worn out shoes when running or exercising. Not warming up properly before exercise. Increasing intensity of exercise too quickly (e.g. running speed or distance covered). Prematurely introducing hill running or stair climbing to exercise routine. Running on hard or uneven surfaces. Calf muscle is injured or has little flexibility (this puts a lot of strain on the Achilles tendon). Sudden intense physical activity such as sprinting for the finish line. Achilles tendinitis can also be caused by differences in foot, leg or ankle anatomy. For example, some people can have flatness in their foot where there would normally be an arch; this puts more strain on the tendon. The FDA has asked that a boxed warning be added to the prescribing information for fluoroquinolone antibiotics. Patients taking these drugs may experience an increased risk of tendinitis and tendon rupture. Fluoroquinolones include Cipro (ciprofloxacin), Factive (gemifloxacin), Levaquin (levofloxacin), Avelox (moxifloxacin), Noroxin (norfloxacin), Floxin (ofloxacin) and Proquin (ciprofloxacin hydrochloride). It is important to remember that the risk for injury is not necessarily gone when the drug is stopped. Cases have been reported in which tendon problems occurred up to several months after the drug was discontinued.
Symptoms
Symptoms of Achilles tendinitis and tendinosis include recurring localized heel pain, sometimes severe, along the achilles tendon during or after exercise. Pain often begins after exercise and gradually worsens. Morning tenderness or stiffness about an inch and a half above the point where the Achilles tendon is attached to the heel bone. Sluggishness in your leg. Mild to severe swelling. Stiffness that generally diminishes as the tendon warms up with use.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
Most of the time, treatment for achilles tendinitis beginning with nonsurgical options. Your CFO physician may recommend rest, ice, ibuprofen, and physical therapy. If after 6 months, the pain does not improve, surgical treatment may be necessary. The type of surgery would depend on the exact location of the tendinitis and extent of damage.
Surgical Treatment
Surgery for an Achilles tendon rupture can be done with a single large incision, which is called open surgery. Or it can be done with several small incisions. This is called percutaneous surgery. The differences in age and activity levels of people who get surgery can make it hard to know if Achilles tendon surgery is effective. The success of your surgery can depend on, your surgeon's experience. The type of surgery you have. How damaged the tendon is. How soon after rupture the surgery is done. How soon you start your rehab program after surgery. How well you follow your rehab program. Talk to your surgeon about his or her surgical experience. Ask about his or her success rate with the technique that would best treat your condition.
Prevention
Achilles tendinitis cannot always be prevented but the following tips will help you reduce your risk. If you are new to a sport, gradually ramp up your activity level to your desired intensity and duration. If you experience pain while exercising, stop. Avoid strenuous activity that puts excessive stress on your Achilles tendon. If you have a demanding workout planned, warm up slowly and thoroughly. Always exercise in shoes that are in good condition and appropriate for your activity or sport. Be sure to stretch your calf muscles and Achilles tendon before and after working out. If you suffer from Achilles tendinitis make sure you treat it properly and promptly. If self-care techniques don?t work, don?t delay. Book a consultation with a foot care expert or you may find yourself sidelined from your favourite sports and activities.